

UN/DESA Policy Brief #69: Leaving no one behind: the COVID-19 crisis through the disability and gender lens

Persons with disabilities—both visible and invisible—face obstacles and discrimination in accessing health care and other essential services, social protection and income security, mental health services, and communication technologies. In addition, women and girls with disabilities are subject to intersecting forms of discrimination related to sexual and reproductive health, gender-based violence, legal protection, unpaid care and domestic work. Women and girls with disabilities who are migrants, refugees, or from ethnic minorities endure even more hardships and unequal treatment. Gender, disability and structural inequalities, which characterized societies before the crisis, are being exacerbated by the multifaceted impact of the COVID-19 crisis. Lack of gender and disability disaggregated data makes it difficult to carry out evidence-based analysis of the socioeconomic impact of the COVID-19 crisis and to facilitate targeted and mainstreamed policies for women and girls with disabilities.
The situation of persons with disabilities through the gender lens
Persons with disabilities face the same risk of infection from COVID-19 as the rest of the population. However, in many cases, the danger posed by the virus is compounded by many other factors. In addition to the disruption of essential services and support, pre-existing health conditions in some cases leave persons with disabilities more at risk of developing serious health conditions.
In general, persons with disabilities have more health care-related needs than others—both standard needs and needs linked to their impairments—and are therefore more vulnerable to the negative impact of low quality or inaccessible healthcare services than those without disabilities. According to the 2018 United Nations Disability and Development Report, among 43 countries with data, 42 per cent of persons with disabilities versus 6 per cent of persons without disabilities perceive their health as poor. Persons with disabilities are often unable to access mainstream healthcare services due to unaffordability, attitudinal barriers, inaccessibility to healthcare facilities, and lack of alternative means to access public health information and communication for those with visual impairments as well as hearing or cognitive disabilities. This pandemic has further intensified the health risks of persons with disabilities who are living in institutional settings.
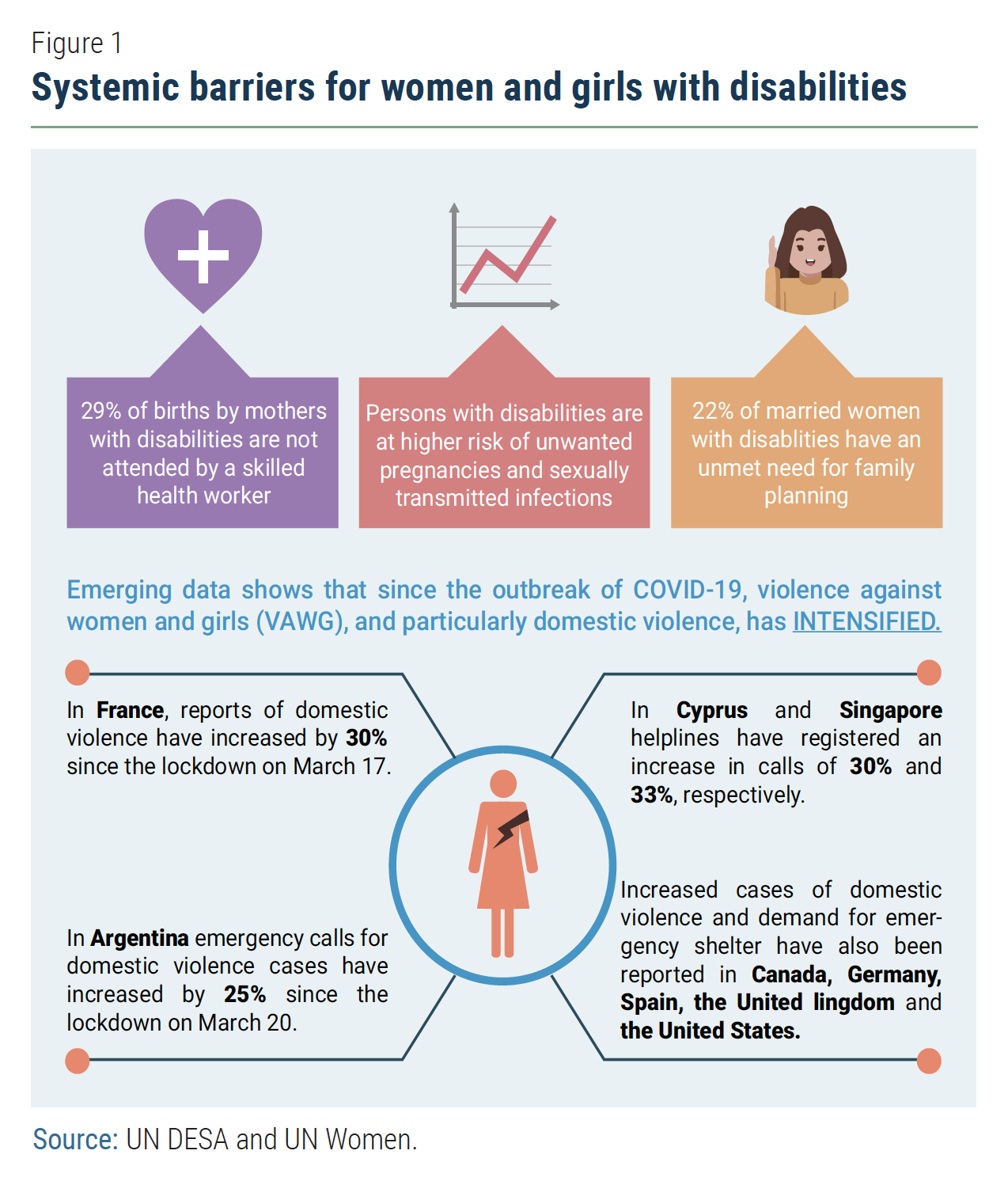
Among those with disabilities, women and girls face systemic barriers to equality and inclusion, with limited visibility in disability and gender equality laws, policies, and practices. Available data suggest that the gap is large compared with men without disabilities: women with disabilities are three times more likely to have unmet needs for health care; three times more likely to be illiterate; two times less likely to be employed and two times less likely to use the internet. Moreover, women with disabilities are at heightened risk of suffering sexual violence compared to those without disabilities.
The COVID-19 crisis exposes these underlying inequalities and exacerbates the situation of women and girls with disabilities. For them, the everyday barriers such as physical accessibility, barriers to implementing basic hygiene measures, affordability of healthcare, limitations on health insurance, and discriminatory laws and stigma, can be life threatening in the midst of a pandemic.
As health emergencies such as COVID-19 place additional pressure on national health services, it is important that national authorities establish non-discriminatory ethical medical guidelines to protect persons with disabilities. The World Health Organization (WHO) has issued disability-inclusive guidelines that are in line with international human rights conventions. Policies and practices on medical treatments, including triage decision-making and access to testing and vaccinations, when available, must not be discriminatory on the basis of age, gender, ethnicity or disability.
Healthcare authorities need to implement proactive accommodation measures that are necessary to reduce the risk of infection for persons with disabilities, their families and care givers, while upholding their dignity and autonomy. Health personnel, including in emergency response services, need to be trained in the challenges facing persons with disabilities during the pandemic and include their needs from the planning stages of such services and not as an afterthought.
Persons with disabilities and their families must be able to continue receiving the same level of care and support, and even more intensively during emergency situations, so that they are able to continue living an independent life. Governments and education providers need to ensure that distance learning platforms are safe and accessible for girls and boys with disabilities, including those with developmental and intellectual disabilities. Specific support should also be provided for caregivers, including access to psychological support.
Build back better
The recovery steps taken today to building back to a better tomorrow will be fundamental to the rights and well-being of women and girls and of persons with disabilities and should take place in line with the United Nations Convention on the Rights of Persons with Disabilities (UN CRPD) and other relevant international norms and standards for the achievement of the goals of the 2030 Agenda for Sustainable Development.
The proportion of persons with disabilities living in poverty is double the proportion of persons without disabilities in some countries, with the challenges compounded further for women and girls. This highlights the imperative need for a social protection system that is gender– and disability-responsive.
Countries that have built social protection systems and have age-, sex- and disability-disaggregated census data and registry-based data are better able to provide universal allowance and support services for a fast and targeted relief. Examples include direct compensation provided to women with disabilities working in the informal economy or to women who care for relatives with disabilities through cash transfers, in-kind support services or priority access to food, housing and other types of support.
Disaggregation of data by sex and disability as well as a systematic gender analysis is thus important; including ensuring tailored support to women and girls to access emergency aid as well as in designing interventions to fight gender-based violence. Information on the programmes and the services to address violence against women and girls should be available to and inclusive of women with disabilities.
Awareness-raising and risk communication strategies need to be specifically targeted to higher risk groups, including women and girls living in precarious conditions. Community-based and locally adaptive approaches to transfer information can be useful to reach women and girls and persons with disabilities who have limited access to technology.
Stakeholders engaged in prevention and recovery, including healthcare workers in hospitals, education providers, disability service providers, protection officers, among others, need to receive guidance and have access to resources that enable them to provide alternative formats and methods of communications, such as sign language. Information should also be age-appropriate, where possible, so children can take the same precautions.
Measures put in place during a pandemic such as rapid upskilling of healthcare workers and equipping healthcare structures that are both gender– and disability-inclusive can help to strengthen national health systems in the long run, which is essential for the overall health and well-being of individuals and societies as envisioned in the 2030 Agenda.
Organizations of persons with disabilities, women’s organizations, and community-based groups of women and women with disabilities serve as indispensable agents and partners to local and national authorities. Together they can ensure that the needs of women and girls and those with disabilities across their diversity are fully included in the planning, monitoring and evaluation of the COVID-19 prevention and building back measures. These organizations play an effective role in promoting gender-and disability-inclusive responses. They can provide practical advice on how to overcome these barriers at national and local levels as well as offer information to persons with disabilities on accessible prevention strategies and support, including on gender-based violence.
The COVID-19 crisis presents a reflective opportunity to strengthen global, local and people-centered recovery actions now in this Decade of Action. The international community should work in solidarity to ensure that societies emerge from the COVID-19 crisis stronger, resilient to future shocks, and more equal and inclusive, in order to achieve a sustainable future for all, including women and girls with disabilities.
Recommendations for the inclusion of persons with disabilities, including women with disabilities, in the response to the COVID-19 crisis
- Consult persons with disabilities and their representative organizations, in particular with organizations of women and girls with disabilities, with regard to COVID-19 containment and mitigation measures to ensure these are disability-inclusive, gender-sensitive and accessible.
- Ensure inclusive, gender-sensitive, accessible and non-discriminatory healthcare to minimize
mortality of those with disabilities and underlying health conditions.- Promote inclusive and accessible treatment and care, including mental health and psychosocial support and care services, in particular for women and girls with disabilities with limited access to
such services; - Establish non-discriminatory ethical medical guidelines to protect persons with disabilities. Policies and practices on medical treatments, including triage decision-making and access to testing and vaccinations, when available, must not be discriminatory on the basis of age, gender, ethnicity or
disability; and - Provide disability sensitivity training to service providers, including public officials and private agencies.
- Promote inclusive and accessible treatment and care, including mental health and psychosocial support and care services, in particular for women and girls with disabilities with limited access to
- Ensure individuals’ health, safety, dignity, and self-autonomy in the community and the continuation of health care support and services for persons
with disabilities and their families for an
independent living.- Implement targeted measures to protect persons with disabilities and those with vulnerabilities living in institutional settings with heightened risk of neglect, restraint, isolation or abandonment.
- Provide solutions for remote work and education that are disability-inclusive and gender-sensitive, such as reasonable accommodation at home and access to adapted and accessible materials.
- Ensure inclusive and non-discriminatory public information and communication to be accessible to all, including to those with limited access to technology.
- Ensure social protection measures are gender– and disability–responsive, and provide targeted financial relief and income support for persons with disabilities and their caregivers who are disproportionately impacted by the crisis.
- Promote disaggregation of data by age, sex and disability and gender analysis of the barriers faced by women and girls with disabilities.
Follow Us